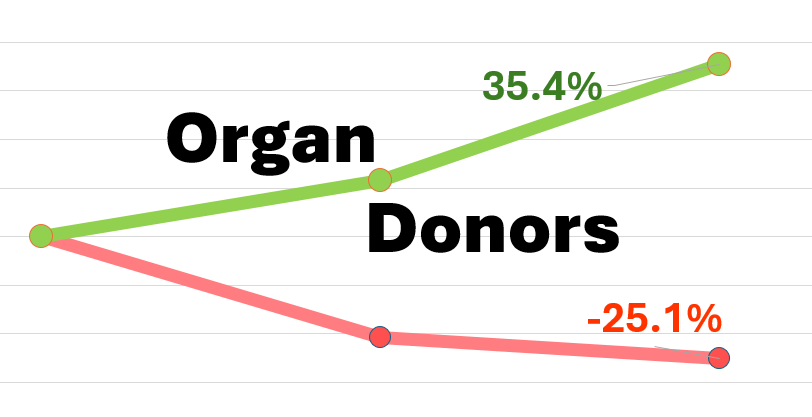
Would you be surprised to learn that the green line above is an OPO projected to be CMS Tier 2 and the red line is an OPO projected to be CMS Tier 1? This makes no sense!
Well, a newly published peer-reviewed study identifies a substantial statistical methodology error in federal regulations that further throws into question the validity of the metric that has already been the subject of significant criticism. This astonishing finding requires immediate action to avoid throwing the national system of organ donation and transplant into chaos come 2026.
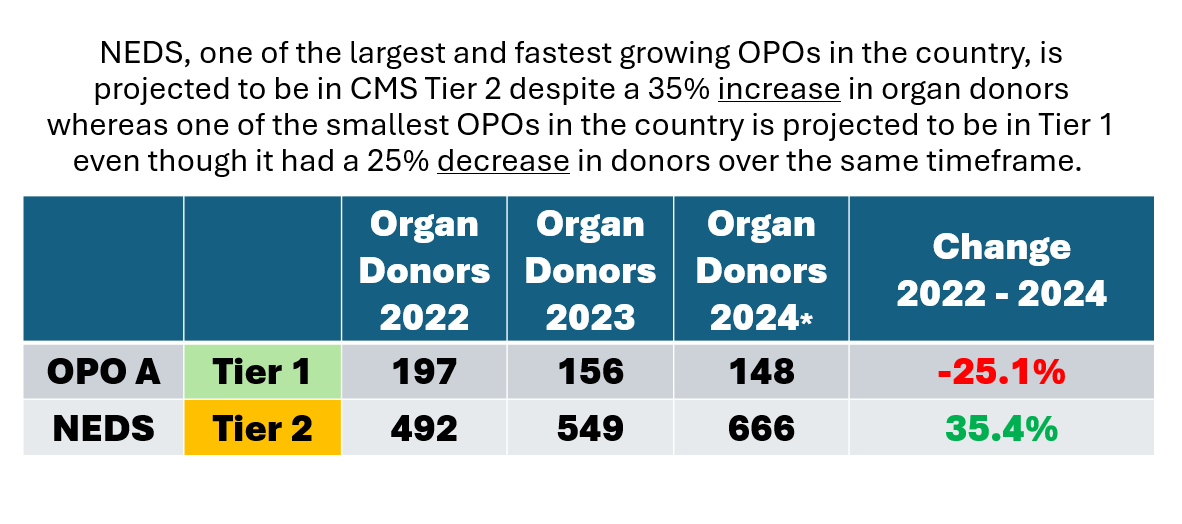
Consider the graphic using projected data below of one of the smallest OPOs in the U.S. that has significantly decreased its performance over the past 3 years and yet remains classified as a Tier 1 OPO under the current regulations versus New England Donor Services, one of the top 3 largest OPOs in the U.S. that has dramatically increased its performance over this same time period and is classified as Tier 2 OPO. Under the current CMS regulations that include a statistically biased methodology, the small Tier 1 OPO with three years of decreasing performance would be recertified, while the large OPO that demonstrated three years of large scale performance improvement would remain at risk of decertification. Troubling.
Current federal regulation purport to assign organ procurement organizations (OPOs) into “performance tiers” with Tier 1 being the top 25%, Tier 2 performing above the median but below the top 25%, and Tier 3 being below the median. As structured, every OPO not in Tier 1 (about 70% of them) will be put at risk for decertification and about 40% of OPOs (assigned Tier 3) will be automatically decertified. However, this new study finds that the statistical method for determining Tier assignment unfairly mathematically benefits the smallest OPOs pushing more of them artificially into the top Tier not based on performance but based on the statistical method used to the detriment of EQUALLY performing large OPOs. The study found that OPOs performing at the same rate can be assigned to different Tiers under the federal regulations methodology solely based on whether they are small OPOs or large OPOs. This means that an OPO may be more at risk for decertification because it is large, not because it is underperforming.
“In conclusion, findings illustrate that current CMS evaluation system appears to be systematically biased against larger OPOs, with smaller OPOs more likely to be automatically recertified or able to compete for contract renewal even when actual performance is equivalent.”
– Association between Organ Procurement Organization Volume
and CMS Performance Evaluations (Rocio Lopez et al. Am J Transplant. 2024)
If left unchanged, the public health system of organ donation in the country’s largest metropolitan areas will be uprooted in 2026 as the federal government begins decertifying community based OPOs as a result of the mistaken statistical methodology. Current projections show that Boston, New York, Los Angeles, Atlanta, Chicago, Houston, Dallas, Minneapolis, Phoenix, Detroit, Seattle, Miami, Washington DC and many other populations could be left without an OPO with local experience to perform the complex work of making organ donation happen for those awaiting transplant.
This study is just the latest evidence that the regulations are deeply flawed. Not only is there a size bias against large volume OPOs, but the regulations are not risk-adjusted for the most common health differences in underlying populations that impact donation/transplant rate such donor age, cause of death and comorbidities – factors over which OPOs have no control. As such, the regulations are not actually measuring OPO performance. Further, the regulations rely on the archaic use of death certificates to estimate the number of medically suitable donors in a service area even though death certificates lack the detailed medical information necessary for this use. And, the regulations do not even take into account whether an OPO has improved its donation and transplant rate over time when evaluating whether to decertify.
As we’ve urged before, the federal government should immediately make changes to the current regulations, modernize them so that OPO are held to actual validated performance standards and not statistically flawed methodologies.
*2024 data projections as of October 31, 2024. optn.transplant.hrsa.gov